



Amylin's Wobbly Tightrope Walk in the Neuroendocrine Circus of Multiple Endocrine Neoplasia
A Delicate Balancing Act:
Multiple Endocrine Neoplasia (MEN) syndromes are a constellation of rare disorders characterized by the uncontrolled growth of tumors in multiple endocrine glands. Amidst this chaotic orchestra of hormonal imbalances, a fascinating molecule named amylin plays a starring role, albeit a precarious one. Its wobbly tightrope walk in the neuroendocrine circus of MEN adds a layer of complexity to this already enigmatic condition.
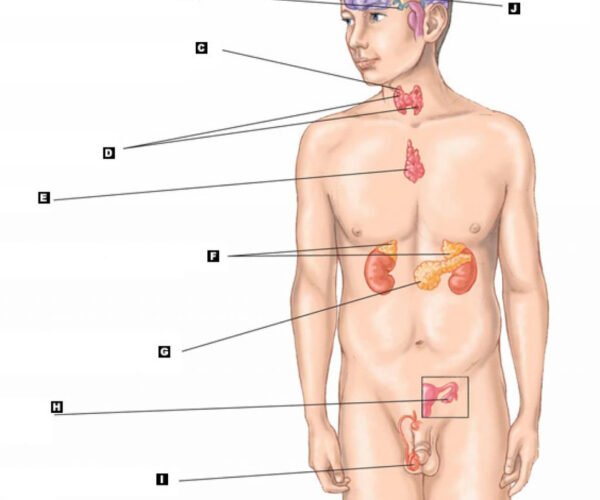
Imagine a Big Top under the searing desert sun. Inside, a whirlwind of activity unfolds. Gigantopithecus-sized pituitary glands spew growth hormone, dwarfing neighboring thyroids churning out an overabundance of thyroid hormones. In the distance, parathyroid glands erupt in volcanic bursts of parathyroid hormone, throwing calcium regulation into disarray. This is the MEN circus, a chaotic microcosm of hormonal imbalance.
And then there’s amylin. Produced alongside insulin by the beta-cells of the pancreas, amylin is a small protein with a big impact. Its primary function is to slow down stomach emptying, ensuring steady blood sugar levels after a meal. In a healthy individual, amylin and insulin form a synchronized duet, maintaining hormonal harmony.
But in the MEN circus, the melody turns discordant. Mutations in genes like RET or MEN1 can disrupt amylin production or processing, introducing unwanted notes into the hormonal score. One consequence is amylin aggregation, where the protein misfolds and clumps together, forming amyloid deposits that can damage pancreatic beta-cells. This, in turn, leads to impaired amylin secretion, adding another layer of dysfunction to the already imbalanced system.
The impact of amylin’s tightrope walk in MEN goes beyond just blood sugar control. Amylin also plays a role in satiety, signaling fullness to the brain and preventing overeating. When amylin malfunctions, the feeling of fullness becomes muted, potentially contributing to the weight gain commonly seen in MEN patients. Additionally, amylin exhibits neuroprotective properties, and its deficiency might contribute to the cognitive and neurological complications sometimes associated with MEN.
Unraveling the complex interplay between amylin and MEN is an ongoing scientific pursuit. Studies suggest that targeting amylin aggregation or enhancing its secretion could hold therapeutic promise. Therapies such as tafamidis, currently used for transthyretin amyloidosis, are being investigated for their potential to stabilize amylin and prevent its aggregation. Additionally, researchers are exploring ways to stimulate amylin production through GLP-1 receptor agonists, medications already used to treat type 2 diabetes.
However, the tightrope amylin walks is fraught with challenges. Targeting amylin without disrupting insulin secretion is crucial, as further impairing beta-cell function could be detrimental. Additionally, the diverse genetic landscape of MEN and the individual variability in amylin’s role within each patient necessitate personalized treatment approaches.
The future of MEN therapy holds the promise of a more nuanced understanding of amylin’s role. By deciphering the intricate dance between this delicate molecule and the hormonal circus of MEN, researchers hope to develop targeted therapies that restore balance and harmony to the lives of individuals affected by this rare and challenging condition.
Delving Deeper into Amylin’s Wobbly Tightrope Walk in MEN:
I understand your request for more details about amylin’s role in MEN. Here’s a deeper dive into the specific mechanisms, clinical implications, and potential therapeutic avenues:
Mechanisms of Amylin Dysfunction in MEN:
- Genetic mutations: Mutations in genes like RET or MEN1 can disrupt amylin’s preproprotein processing, leading to altered peptide fragments with reduced efficacy or aggregation-prone characteristics.
- Endoplasmic reticulum stress: The overproduction of hormones in MEN can overwhelm the protein folding machinery in the endoplasmic reticulum (ER), promoting amylin misfolding and aggregation.
- Proteasomal dysfunction: Mutations in MEN genes can also impair the proteasome, the cellular machinery responsible for degrading misfolded proteins, leading to the accumulation of amyloid deposits.
Clinical Implications of Amylin Dysregulation:
- Impaired gastric emptying: Reduced amylin secretion leads to faster stomach emptying, resulting in postprandial blood sugar spikes and increased risk of hypoglycemia.
- Altered satiety signaling: Deficient amylin signaling blunts the feeling of fullness, potentially contributing to weight gain and metabolic complications.
- Neuroendocrine symptoms: Some studies suggest a link between amylin deficiency and the neurological and cognitive issues sometimes observed in MEN patients.
- Amyloid neuropathy: Accumulation of amyloid deposits in peripheral nerves can lead to pain, numbness, and other neuropathic symptoms.
Potential Therapeutic Strategies:
- Amyloid stabilization: Tafamidis and other stabilizers are being investigated to prevent amylin aggregation and protect beta-cell function.
- GLP-1 receptor agonists: These drugs stimulate GLP-1 receptors, which in turn can enhance amylin secretion and improve glucose control.
- Beta-cell preservation: Therapies promoting beta-cell survival and regeneration could indirectly address amylin deficiency by protecting the cells that produce it.
- Personalized medicine: Understanding individual variations in amylin function within different MEN subtypes will be crucial for tailoring treatment strategies.
Empowering Minds, Nourishing Bodies: Introducing Hormone.
In the pursuit of knowledge-driven wellness, Dr. Zaar, a distinguished specialized clinic dietitian in Lahore, introduces a groundbreaking educational initiative—Hormone.
Read MoreDopamine and the Unsustainable Pursuit of.
In the fast-paced corporate world, the quest for success often turns into a relentless chase for a ‘high.’ This chase.
Read More