



Prolactin Dysfunction in Diabetes Mellitus: Exploring the Hormonal Imbalance
Case Study: Prolactin Dysfunction in a Patient with Diabetes Mellitus
Patient Profile: Mrs. Anderson, a 52-year-old female, was diagnosed with Type 2 Diabetes Mellitus (T2DM) five years ago. Despite adherence to prescribed medications and lifestyle modifications, her glycemic control remained suboptimal. Intrigued by the complexity of diabetes, her endocrinologist decided to investigate the potential role of hormonal imbalances, specifically focusing on prolactin levels.
Clinical Presentation: Mrs. Anderson’s initial presentation included elevated fasting blood glucose levels, insulin resistance, and fluctuations in weight. Despite rigorous efforts to manage her diabetes, the patient experienced persistent challenges in achieving glycemic control. The endocrinologist, suspecting a hormonal component in her case, decided to delve deeper into the role of prolactin.
Investigations: Laboratory tests revealed elevated prolactin levels, indicating potential prolactin dysfunction. Further investigations aimed to explore the connection between prolactin and diabetes mellitus. Results showed evidence of impaired insulin sensitivity and beta-cell dysfunction, aligning with the literature on prolactin’s impact on glucose metabolism.
Additionally, markers of chronic inflammation were elevated, suggesting a potential link between prolactin and the inflammatory milieu observed in diabetes. Adipokine dysregulation, particularly altered levels of leptin and adiponectin, pointed towards the involvement of prolactin in adipose tissue dysfunction, contributing to insulin resistance.
Treatment Approach: Armed with the insights gained from the investigations, Mrs. Anderson’s treatment plan was adjusted to address the prolactin dysfunction alongside conventional diabetes management. The endocrinologist prescribed medications targeting prolactin levels, aiming to restore hormonal balance and improve insulin sensitivity.
Lifestyle modifications were also emphasized, with a focus on dietary changes and increased physical activity. The patient was educated about the potential impact of prolactin on her diabetes and the importance of a comprehensive approach to address both hormonal and metabolic aspects of the condition.
Outcome: Over the course of several months, Mrs. Anderson’s response to the adjusted treatment plan was monitored. Regular follow-up assessments revealed improvements in glycemic control, insulin sensitivity, and inflammatory markers. The patient reported a more stable weight, and her overall well-being showed positive signs of enhancement.
By addressing prolactin dysfunction alongside conventional diabetes management, Mrs. Anderson’s case highlighted the importance of considering hormonal imbalances in the comprehensive care of individuals with diabetes mellitus. This personalized approach, tailored to the patient’s specific hormonal profile, showcased the potential benefits of a nuanced treatment strategy.
Conclusion: The case of Mrs. Anderson underscores the significance of recognizing and addressing prolactin dysfunction in patients with diabetes mellitus. By incorporating hormonal considerations into the diagnostic and therapeutic framework, healthcare professionals can offer more personalized and effective management strategies, ultimately improving outcomes for individuals with this complex metabolic disorder. Further research is warranted to refine our understanding of the interplay between prolactin and diabetes, paving the way for innovative and targeted therapeutic interventions.
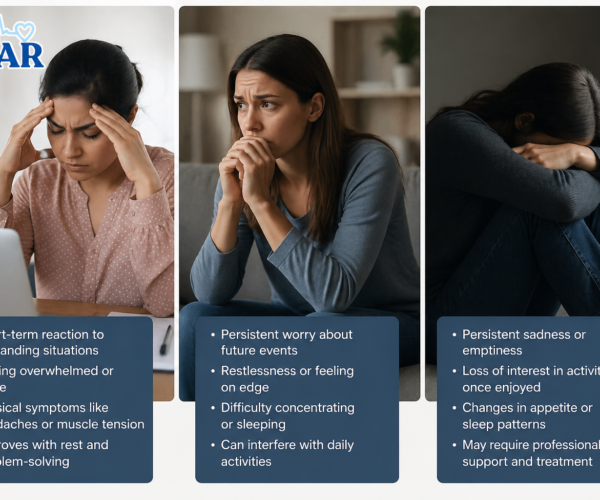
Difference Between Stress Anxiety and Depression.
Knowing how to tell the difference between stress anxiety and depression is important, considering that there are many people who.
Read More
Height Clinic: Elevate Confidence on Your.
In a world where confidence often goes hand in hand with stature, the quest for height enhancement has led many.
Read More